Oral rehabilitation case with fixed prosthesis with STRATEGIC IMPLANT

Clinical Case of STRATEGIC IMPLANT.
ORAL REHABILITATION WITH FIXED PROSTHESIS ON IMPLANTS IN THE JAW
VERY ATROPHIC WITH BASAL IMPLANTS AND SINGLE-PHASE IMPLANTS.
Author: Dr. Miguel Alvarado Pastor
SUMMARY
Clinical case with Strategic Implant ®
This article shows how to solve with an “Immediate Load” implant treatment the case of a patient with a very advanced alveolar atrophy in both jaws, applying the rules of Strategic Implantology developed by Dr. Stefan Ihde y Cols. at the International Implant Foundation (IF). In this case it was decided to place “Strategic Implants ® ” in the upper jaw of the BCS ® model of Ø 3.5 and lengths 17,14,14 and 10 mm and of the ZSI ® model of Ø 4.6 and length 50 mm. In the lower jaw it was decided to place single-phase KOS ® and KOS B ® implants of Ø 3.0 – 3.2 – 3.7 and 4.1 in lengths of 12, 15, 10 and 6 mm. All implants are manufactured in Ti6AI4V (Ihde Dental AG). The use of these types of implants allows the rehabilitation of patients with very atrophic jaws.
Following the rules of “Strategic Implantology” it was possible to rehabilitate the patient without having to perform sinus elevations, bone grafts or lateralization of the tooth. In addition to returning the patient’s teeth immediately, thus restoring chewing function, phonetics and, of course, aesthetics on the same day with provisional resin teeth, the definitive zirconium prosthesis was placed after 4 days, and the patient did not have to wait 9 months or more if treatment had been carried out using a traditional approach.
The speed of the treatment, not having to go through bone grafting operations, breast lifts, lateralisation of the teeth and a high level of aesthetics was greatly appreciated by the patient.
INTRODUCTION:
Rehabilitations of patients with very atrophic jaws involve treatments of a high degree of difficulty to rehabilitate with traditional biphasic implants. In addition, these are patients who have been evicted for implants on most occasions (they have been told that they cannot have implants because of lack of bone) or who have to undergo long and painful interventions, such as block bone grafts, sinus elevations or lateralisation of the teeth, with the risks that these entail.
What patients demand from us more and more is immediate solutions, as painless as possible and with the least morbidity, as well as being able to optimise costs.
In this article I intend to show the innumerable advantages of following the philosophy of working with Strategic implant ®, which breaks with the rules and dogmas powerfully established in oral implantology, improving what already exists, innovating and, of course, not replacing it. In summary, these are the concepts of Strategic Implant® :
Discipline and protocol in the manufacture of the prosthesis:
The prosthesis must follow some very easy but strict parameters, such as: splinting of the implants as soon as possible by means of a rigid structure, shape of the prosthetic pieces rounded without very marked edges and, of course, a very stable occlusion, leaving the posterior areas free or in nanoclusion. And all this in record time…
Surgery as the basis of the main work:
All surgery, whatever it may be, must always be very well planned, but with Strategic Implant ® we must also be aware that we are working with atrophied jaws and basal bone, where the measurements of the implants and their location are fundamental to the success of the treatment. In addition, we must have a high level of anatomical knowledge of the jaws, in order to search for an anchorage in the second or third cortices of the implants and to reach them safely, creating a structural polygon between the implants for the subsequent support of the forces exerted by the prostheses.
CLINICAL CASE
43 year old female patient, without systemic diseases, who asks us for rehabilitation with implants. During the exploration the patient presents the 1st and 3rd edentulous quadrant, fixed prosthesis from the 12th to the 28th and another fixed prosthesis bridge from the 34th to the 45th and then 3 biphasic with cemented crowns in the shape of premolars reaching the height of 47-48.

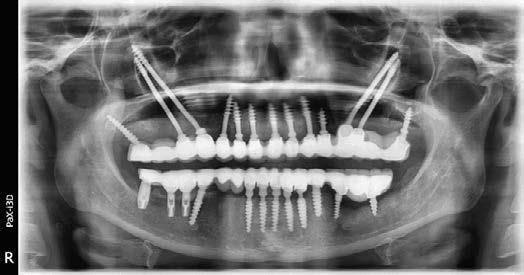
In orthopantomography, a large amount of bone atrophy, root remains and infectious processes can be seen in some pieces. The patient states that she is very unhappy with the aesthetics of her prosthesis, in addition to the discomfort caused by the leaks and the bad odours that emanate from it, she also confesses that she is unable to wear both removables because they cause her nausea. All this makes her request the treatment with implants.
The patient had previously consulted different professionals who had told her that she was not a candidate for rehabilitation with implants or that she had to undergo pre-implant operations (bilateral sinus lift, block bone grafting and possible lateralisation of the tooth in the 3rd quadrant). Another solution given to her was to place 6 implants in the upper jaw and 4 in the lower jaw, rehabilitating with two hybrid prostheses, which the patient immediately discarded due to their characteristics.
The following treatment was decided on: exodontia of all the teeth and root remains, as almost all the teeth are very deteriorated due to filtrations, use the 3 biphasic implants which are currently in good condition, and place Basal Implants following the rules of Strategic Implant ® in the upper jaw (BCS ® and Zygomatic ZSI ® – Ihde Dental AG) and in the lower jaw single-phase implants (KOS ® and KOS B ® – Ihde Dental AG). Plus an immediate provisional resin prosthesis and later a definitive zirconium prosthesis.
METHOD AND MATERIALS
The patient is given an upper and lower CT scan, study models and records are taken for the preparation of the provisional ones, so that they are available on the day of surgery.
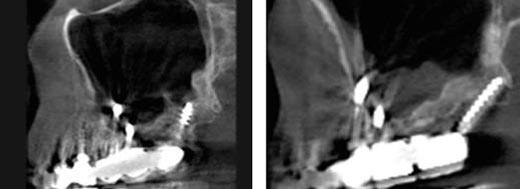
On the day of surgery, the teeth are exodonted and 7 BCS ® strategic implants are placed in the previous group, 5 of which seek anchorage in the floor of the nostrils and 2 in the canine eminences.
4 Zygomatic ZSI ® strategic implants are placed (2 in the right side and 2 in the left side), and in the 2nd quadrant at the height of the tuberosity a BCS ® strategic implant with anchorage in the cortical of the sinus floor and the tuberosity, on the other hand in the 1st quadrant at the height of the tuberosity a KOS ® monophase implant was placed looking for anchorage in the wings of the pterygoid.

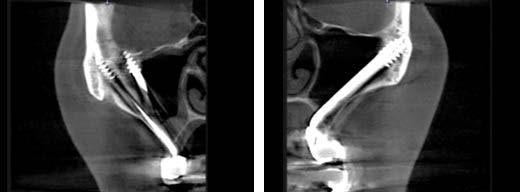
The ZSI® strategic zygomatic implants have a totally polished surface, a Ø 4.6, and lengths that go from 35 to 55, these characteristics allow us to place implants looking for the anchorage in the zygoma, through the breast without causing great destruction of it, causing the minimum inflammation, thus facilitating a fast recovery and also achieving with these implants a very strong and safe anchorage to totally rehabilitate the patient with his fixed prosthesis.
In the lower maxilla we proceeded to perform the exodontia of the teeth and we took advantage of the 3 biphasic implants that the patient was already carrying. First 6 KOS ® implants were placed in the previous group and then another 2 in the 3rd quadrant and 1 more in the 4th quadrant.
Once all the implants were in place, the abutments were ground to make them as parallel as possible. The impressions and records were taken for the production of the fixed prosthesis.
Then the provisional one was trimmed, the occlusion adjusted and cemented. During the remaining 4 days, tests were made of the cap, sponge, occlusion adjustments, finishing and cementing of the definitive zirconium prosthesis, with the occlusion following the rules of Strategic Implantology. Subsequently, the appropriate radiographic controls are carried out, as well as possible occlusion adjustments.



DISCUSSION
It is clear that one does not get up one morning and start performing upper and lower rehabilitations with strategic implants (basal and zygomatic) in patients with atrophied jaws. This is a long road, in which one learns from his mistakes and above all from our patients, but following the steps of Strategic Implant ® I am totally convinced that through this new didactic and pedagogical approach to rehabilitate with implants, one always looks ahead, that everything we can imagine ends up becoming reality in a simple way: implants that the neck can be bent to facilitate the axis of insertion of the prosthesis, implants long enough to be able to take advantage of the best available bone, anchoring themselves even to cortices that are difficult to access. In addition, the fact that your body can be bent allows us to make better use of the anatomical repairs or avoid them so as not to damage them. This is without forgetting its totally polished surface, which makes it impossible for bacteria to adhere to the implants.
In Strategic Implantology it is necessary to have a clear idea of where to place the implants, actively seeking the best available bone, bone the best and most stable anchorage areas of the 2nd and/or 3rd cortices, thus improving the areas of load transmission, by creating a support polygon in which the slopes of the occlusal surfaces of the prostheses are part of the load transmission together with the implants and their position in the bone, all of which closely form strategic positions (hence the meaning of the name “Strategic Implantology”) that favour the success of the treatment. The combination of all these fragments is designed to adapt to a living form that constitutes a whole, as it is; the bone, the forces of mastication and how these are transmitted by the implants and in turn to the skeletal architecture of the jaws.
When I sit down with the patient to plan everything, after seeing all the possibilities and listening to their expectations, I like to explain to them that we are going to carry out a living geometric rehabilitation, which actively adapts to their conditions, in an autonomous, guided way and in a very simple and direct manner.
SUMMARY
The evolutionary step to “Immediate Loading” is to carry out the rehabilitations of our patients with the guidelines of Strategic implant ®, which guarantee and minimize the risks, increasing the success and satisfaction of our patients in a safe and calm manner. It is evident that this leads to a long and hard learning path, but not impossible, and in any case similar or simpler than others (e.g.: grafts). The philosophy and systematic of Strategic Implant ® is based on the scientific evidence of the Immediate Load implants made by Dr. Stefan Ihde y Cols. at the International Implant Foundation (IF), counting for this with a long biography and with innumerable cases and research works made all over the world, which provide a high content of clinical experience and scientific knowledge, which has simplified the technique enormously and has organized the pedagogy to transmit it to the scientific world of health.
Perhaps the most important change is to be able to change in our minds as health professionals, that all our patients can wear implants and that it is not necessary to perform bone grafts on our patients, means breaking rules and principles that are deeply rooted in our daily lives.
Strategic Implant ® provides us with the necessary tools to be able to be number 1 or 2 in our area in order to provide the best service to our patients and also to be able to differentiate ourselves from the rest of the professionals.
You cannot forget your beginnings, always in a haze, with caution, with fear and learning a lot from our failures, until one day someone comes along and clears your horizon completely. Strategic Implant ® revolutionised my way of rehabilitating my patients, eternally grateful for everything it teaches me, but who I think should be much more grateful are my patients to whom without the guidelines of Strategic implant ® I could never have rehabilitated them in such a satisfactory way for them, carrying out rehabilitations that adapt to each one of them in an active, autonomous and totally guided way in an easy and direct way.
Living geometric restorations, so we feel them as a patient and a servant, one more step of Strategic Implant ®.
Bibliography
- Ihde & Ihde. Introduction to Working with Strategic Implant 1. International Foundation Publishing. 2015.
- Ihde & Ihde. Chewing Recipes Book 4. International Foundation Publishing. 2015.
- Ihde & Ihde. Laboratory Work in Strategic Implants 6. International Foundation Publishing. 2016.
- New Systematic Terminology of Cortical Bone Areas for Osseofixed Implants in Implantology Stefan Ihde, Antonina Ihde, Valeriy lysenko, V. Konstantinovic, Lukas Palk.